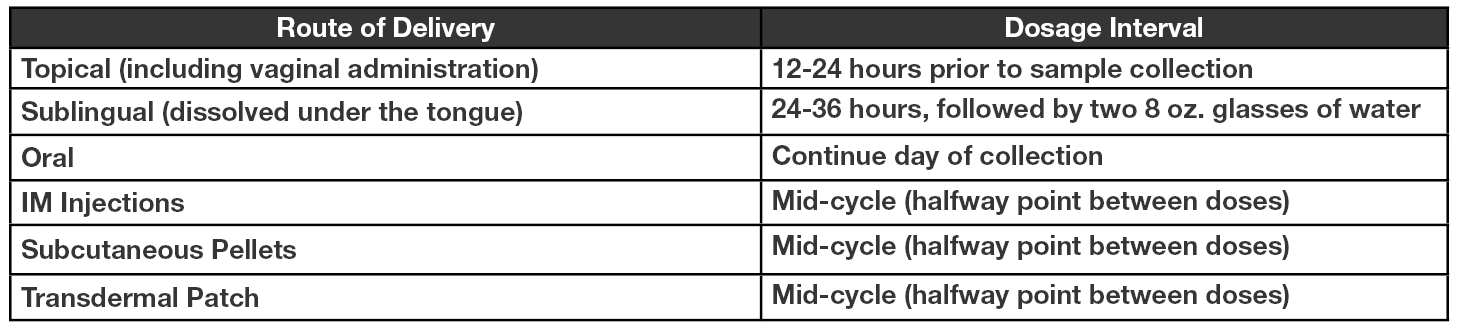
Topical (including vaginal administration): The ideal dosage interval is 12-24 hours before sample collection (the time between last hormone application and first morning sample collection should be 12-24 hours). DO NOT APPLY ANY TOPICAL HORMONES THROUGHOUT THE ENTIRE DAY OF COLLECTION, RESUMING USE AFTER THE 4TH SAMPLE HAS BEEN COLLECTED.
Note: For dosages typically applied at bed-time, refrain from use the evening prior to sample collection or use topical formulation earlier in the day if the period between application and sample collection will be less than 12 hours; i.e.: 6:00 PM application for a 7:00 AM wake-up/morning sample collection (giving a 13 hour dosage interval).
Sublingual (dissolved under the tongue): The interval between last hormone usage and first AM salivary sample collection should ideally be 24 to 36 hours. After the last dose of the hormone has dissolved in the mouth, it should be followed by two 8 oz glasses of water to clear the mouth of any residual hormone. The first saliva sample should then be collected 24 - 36 hours later. DO NOT USE ANY SUBLINGUAL HORMONES THROUGHOUT THE ENTIRE DAY OF COLLECTION. RESUME USE AFTER THE 4TH SAMPLE HAS BEEN COLLECTED.
Note: Residual contamination is often observed in samples with dosage intervals under 24 hours.
Oral: It is recommended to continue PO supplementation as prescribed on the day of collection.
IM Injections: The recommended dosing interval for IM hormones is mid-cycle. For example, the ideal sample collection day for hormone(s) injected every two weeks (14 days) is 7 days after injection.
Subcutaneous Pellets: The recommended dosing interval for subcutaneous pellets is mid-cycle. For example, the ideal sample collection day for pellets that are replaced every 90 days is approximately day 45.
Transdermal Patch: Though the hormone in a transdermal patch is formulated for continual release, a tapering of dose does occur. Therefore, the recommended dosage interval for transdermal patches is mid-cycle. For example, if a patch is replaced weekly (every 7 days) ideal sample collection should occur approximately 3-4 days after application.
Cortisol/Glucocorticoid Supplementation: Due to the short half life of oral cortisol/hydrocortisone with a peak and return to baseline within 1-3 hours; it is difficult to measure therapeutic levels. Therefore it is recommended to evaluate endogenous production which requires discontinuing ALL cortisol supplementation (including inhalers and topical creams) 4-5 days prior to sample collection.
Melatonin Supplementation: Last dose should be at least 36 hours before first saliva sample collection.
Adhering to recommended dosage intervals for saliva testing is a reliable way to ensure accurate results. When patients adhere to these recommendations, providers are best able to monitor the therapeutic response and provide recommendations for supplementation updates as needed. Needless retesting can be avoided by following these guidelines, creating an easy flow of testing and results for both patient and provider.